Case 6: AML with Inversion 16

Inversion of chromosome 16 is associated with acute myeloid leukemia with abnormal eosinophils
These abnormal eosinophils have mixed eosinophilic and basophilic granules
How is the cytogenetic abnormality determined diagnostically?
A brief introduction to cytogenetics…
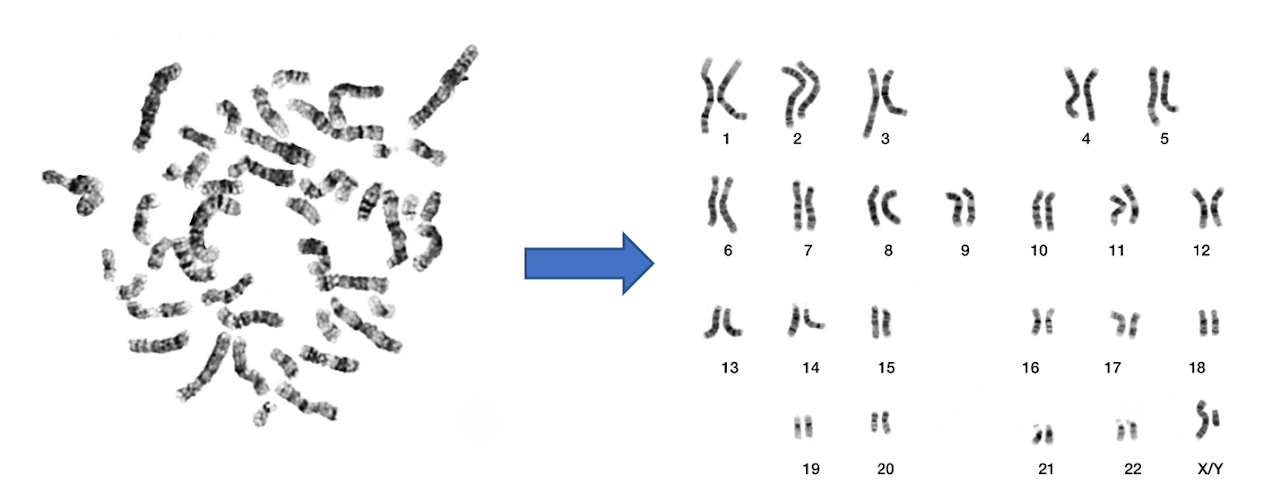
Cytogenetics is the microscopic investigation of the DNA structure/content at the chromosomal level using banding of metaphase preparations
Banding = darker and lighter areas on a chromosome, which are reproducible across specimens
Most common type of banding is G-banding:
- Dark bands: AT-rich, heterochromatic, fewer active genes
- Light bands: CG-rich, euchromatic, more active genes
From Wikipedia ⬇️
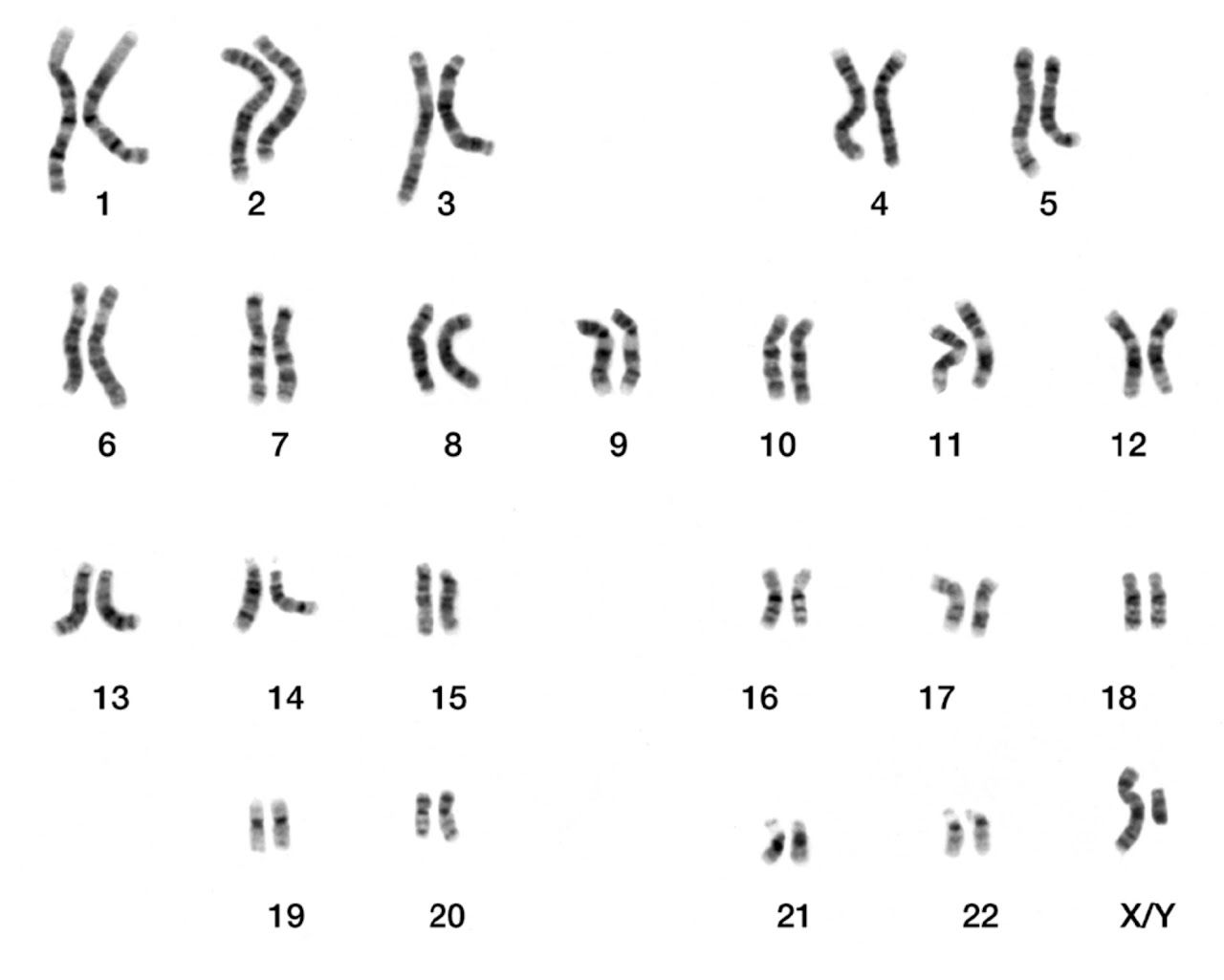
Our talented technologists identify banded chromosomes by assessing (in order):
- Chromosome size
- Centromere position
- Banding pattern
From ASH and Wikipedia ⬇️
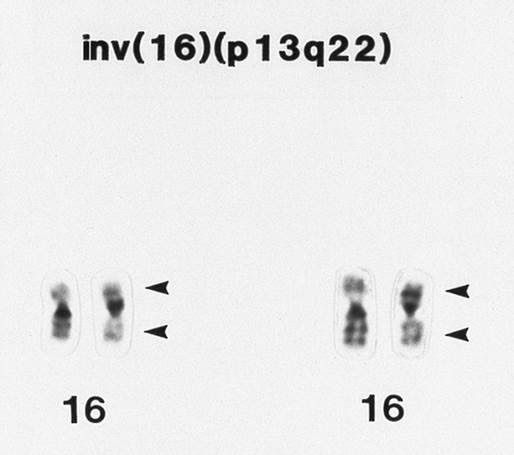
Cytogenetics studies are essential in making a diagnosis of AML with inv 16
This can be subtle on conventional karyotype, so further testing with FISH/molecular is warranted if the karyotype is normal but the morphology suggests inv 16
From PEIR @UABPathology ⬇️
Molecular Pathogenesis
The inversion of chromosome 16 (or the translocation t(16;16) leads to the fusion of CBF-beta and MYH11.
CBF normally binds to enhancers/promoters of genes involved in hematopoiesis, increasing transcription of these target genes, leading to hematopoietic differentiation/maturation
With the fusion gene, this process is blocked ➡️ less transcription of target genes ➡️ less hematopoietic differentiation/maturation ➡️ disease
Finally, it's important to note that AML with inversion 16 is considered to be in the favorable risk category
That's all for today. Thanks for following along!
Find this case on Twitter:
🩸#HemePath AML subtype #PathTweetorial 🧵
— Clarissa E. Jordan, MD (@pathcejmd) March 2, 2022
Which cytogenetic/molecular finding is most consistent with this morphology? (Poll⬇️)#PathTwitter #MolecularPath #MedEd @MayoClinicPath
(P.S. Always learning - I welcome any feedback!) pic.twitter.com/4PUG0ruJq5